
Pancreatic Cysts
What are pancreatic cysts?
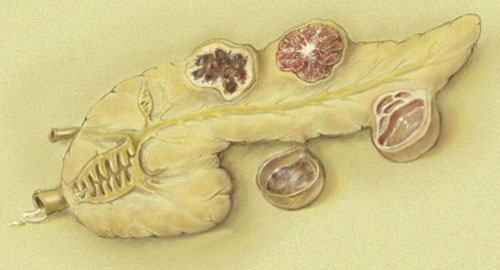
Pancreatic cysts are collections (pools) of fluid that can form within the head, body, and tail of the pancreas. Some pancreatic cysts are true cysts (non-inflammatory cysts), that is, they are lined by a special layer of cells that are responsible for secreting fluid into the cysts. Other cysts are pseudocysts (inflammatory cysts) and do not contain specialized lining cells. Often these pseudocysts contain pancreatic digestive juices because they are connected to the pancreatic ducts. Pancreatic cysts can range in size from several millimeters to several centimeters. Many pancreatic cysts are small and benign and produce no symptoms, but some cysts become large and cause symptoms, and others are cancerous or precancerous. (Precancerous cysts are benign cysts that have the potential to become cancerous.)
Different types of cysts contain different types of fluids. For example, pseudocysts that form after an attack of acute pancreatitis contain digestive enzymes such as amylase in high concentrations. Mucinous cysts contain mucus (a proteinaceous liquid) produced by the mucinous cells that form the inside lining of the cyst.
What are the symptoms of pancreatic cysts?
- The symptoms of pancreatic cysts depend on their size and location. Small (less than two cm) cysts usually cause no symptoms. Large pancreatic cysts can cause abdominal pain and back pain presumably by exerting pressure on the surrounding tissues and nerves.
- Small or large cysts in the head of the pancreas also may cause jaundice (yellowing of the skin and eyes with darkening of the urine) due to obstruction of the common bile duct. (Obstruction causes bile to back up and forces bilirubin–the chemical that produces jaundice–back into the bloodstream and forces it to be excreted in the urine.)
- If the cysts become infected, it may result in fever, chills, and sepsis.
- On rare occasions, large pseudocysts can compress the stomach or the duodenum leading to obstruction to the movement of food in the intestines, resulting in abdominal pain and vomiting.
- If a cyst becomes malignant and begins to invade the surrounding tissues, it may lead to the same type of pain as pancreatic cancer, pain that usually is constant and felt in the back and upper abdomen.
What are the causes of pancreatic cysts?
There are two major types of pancreatic cysts; pseudocysts (inflammatory cysts) and true cysts (non-inflammatory cysts). Inflammatory cysts are benign, whereas non-inflammatory cysts can be benign, precancerous, or cancerous.
Pseudocysts
Most of the inflammatory cysts of the pancreas are pancreatic pseudocysts. Pseudocysts of the pancreas result from pancreatitis (inflammation of the pancreas). The common causes of pancreatitis include alcoholism, gallstones, trauma, and surgery. The fluid inside the pseudocysts represents liquefied dead pancreatic tissue, cells of inflammation, and a high concentration of digestive enzymes that are present in pancreatic exocrine secretions. (Most pseudocysts have connections with the pancreatic ducts.) Most pseudocysts caused by acute pancreatitis resolve spontaneously (without treatment) within several weeks. Pseudocysts that need treatment are those that persist beyond six weeks and are causing symptoms such as pain, obstruction of the stomach or duodenum, or have become infected.
True cysts
- Serous cyst adenomas: These cysts are mostly benign and commonly occur in middle-aged women. They usually are located in the body or tail of the pancreas. Typically they are small and cause no symptoms although rarely they may cause abdominal pain.
- Mucinous cyst adenomas: Thirty percent of these cysts contain cancer, and those that do not contain cancer are considered precancerous. They also commonly occur in middle-aged women and are usually located in the body or tail of the pancreas.
- Intraductal papillary mucinous neoplasm (IPMN): These cysts have a high likelihood of being or becoming cancerous. At the time of diagnosis, there is a 40% to 50% chance of the cyst already being cancerous. These cysts are more common in middle-aged men and are more commonly located in the head of the pancreas. The cysts typically produce large amounts of mucous which sometimes can be seen draining out of the papilla of Vater at the time of endoscopic retrograde cholangio-pancreatography (ERCP), a test that visualizes the ampulla of Vater and the pancreatic duct. These cysts can cause abdominal pain, jaundice, and pancreatitis. Increased risk for cancer occurs with older age of the patient, presence of symptoms, involvement of the main pancreatic duct, dilation of the main pancreatic duct over 10 mm, the presence of nodules in the wall of the duodenum, and size over 3 cm for side-branch IPMN.
- Solid pseudopapillary tumor of the pancreas: These are rare tumors that have both solid and cystic components and are found mainly in young Asian and black women. They may reach a large size and can become malignant. Prognosis is excellent after complete surgical resection of these tumors.
How are pancreatic cysts diagnosed?
Since the majority of pancreatic cysts are small and produce no symptoms, they often are discovered incidentally when abdominal scans (ultrasound [US], computerized tomography or CT, magnetic resonance imaging or MRI) are performed to investigate unrelated symptoms. Unfortunately, ultrasound, CT, and MRI cannot reliably distinguish benign cysts (cysts that usually need no treatment) from precancerous and cancerous cysts (cysts that usually require surgical removal).
Endoscopic ultrasound (EUS) is becoming increasingly useful in determining whether a pancreatic cyst is likely to be benign, precancerous, or cancerous. During endoscopic ultrasound, an endoscope with a small ultrasound transducer at its tip is inserted into the mouth and is passed through the esophagus, and stomach into the duodenum. From this location, which is very close to the pancreas, liver, and gallbladder, accurate and detailed images can be obtained of the liver, pancreas and the gallbladder.
During endoscopic ultrasound, fluid from cysts and samples of tissue also can be obtained by passing special needles through the endoscope and into the cysts.
The fluid obtained by FNA can be analyzed for cancerous cells (cytology), amylase content, and for tumor markers. Tumor markers, such as CEA (carcinoembryonic antigen), are proteins produced in large quantities by cancer cells. For example, pancreatic pseudocyst fluid will typically have high amylase levels but low CEA levels. A benign serous cyst adenoma will have low amylase and low CEA levels, whereas a precancerous or cancerous mucinous cyst adenoma will have low amylase levels but high CEA levels. Most recently, DNA from cells that are aspirated from the cyst has been analyzed for changes suggestive of cancer.
The risks of endoscopic ultrasound and fine needle aspiration are small and consist of a very small incidence of bleeding and infection.
Occasionally, it is difficult even with the diagnostic tools of endoscopic ultrasound and fine needle aspiration to determine if a pancreatic cyst is cancerous or precancerous. If the answer is not clear, sometimes repeated endoscopic ultrasound and aspiration are done if the suspicion for cancer or precancer is high. In other cases, the cyst is reexamined by CT, MRI, or even endoscopic ultrasound after a few months to detect changes that more strongly suggest that cancer has developed. In still others, surgery is recommended.
What is the treatment for pancreatic cysts?
The most important aspect of management of pancreatic cysts is the determination of whether a cyst is benign (and usually needs no treatment) or if it is precancerous or cancerous and must be removed.
The second most important aspect of management is to determine whether a patient with a precancerous or cancerous pancreatic cyst is a suitable surgical candidate. In medical centers experienced in performing pancreatic surgery, surgical removal of precancerous or cancerous cysts results in a high rate of cure.
Very small cysts can be followed to detect an increase in size that may indicate cancer or an increased risk of developing cancer. Not all cysts need to have endoscopic ultrasound or be aspirated; some may have characteristics so suggestive of malignancy that surgery is recommended without endoscopic ultrasound. Others may have characteristics so suggestive of a non-cancerous cyst that no endoscopic ultrasound needs to be done although imaging studies (ultrasound, CT, MRI) may be repeated periodically. There are not yet standard recommendations for managing pancreatic cysts.
-
Pancreatic pseudocysts need treatment if they persist beyond six weeks after acute pancreatitis, especially if they reach a large size and cause symptoms such as obstruction of the stomach or common bile duct, abdominal pain, or become infected. Small pancreatic cysts (for example, cysts smaller than one cm) will have little chance of being cancerous. Nevertheless, even these small cysts can grow in size and turn cancerous in the future. Thus, these patients are monitored with yearly scans (for example, yearly ultrasound or MRI). The cysts do not have to be evaluated with endoscopic ultrasound and fine needle aspiration. If the cysts grow in size and/or cause symptoms, the patient will be evaluated further using endoscopic ultrasound and fine needle aspiration.
-
Pancreatic cysts larger than 2 cm in young, healthy individuals usually are treated with surgical removal, especially if the cysts produce symptoms.
-
Pancreatic cysts larger than 2 cm in elderly patients can be studied with endoscopic ultrasound and fine needle aspiration. If fluid cytology, CEA measurements or analysis of DNA suggest cancerous or precancerous changes, the patients can be evaluated for pancreatic surgery.